

In the first part, we discussed the option of an oral cycle for beginners. In this part, we’ll go over the injectable cycle — which is actually the best choice for a beginner, even though oral cycles are not a bad option, provided they are properly structured.
The best choice for a first injectable cycle is an injectable testosterone (TST), and there is no need to add any other AAS to it. During this cycle, you will be able to observe your body’s reaction to testosterone, determine the level of oestrogenic activity, and assess your tolerance to increased DHT levels and other possible side effects.
There are several forms of injectable testosterone available on the market:
Testosterone without ester
Testosterone Propionate (half-life: 1–2 days)
Testosterone Enanthate (half-life: 4–5 days)
Testosterone Cypionate (half-life: 5–6 days)
Sustanon (a mix of esters, half-life up to 21 days)
Testosterone Undecanoate (half-life: 16–34 days)
The question is — which one to choose, which is the most suitable for a beginner, and why? Let’s go through all these forms briefly and clearly so you can make an informed choice.

1. Testosterone without ester
Not suitable for beginners — although it has a very fast onset of action, the fact that it has no ester attached means it must be injected several times a day.
There’s no need to go into more detail, as this form of testosterone is intended mainly for experienced users and has its own specific applications.
2. Testosterone Propionate
Not a bad choice, but it has a short half-life and therefore needs to be injected every day or every other day, which most beginners dislike because it’s uncomfortable and inconvenient.
3. and 4. Testosterone Enanthate and Cypionate
These are the best options for beginners. They can be injected once every 3 to 7 days.
Experienced users tend to inject every 3–4 days, while beginners usually go for every 5, 6, or even 7 days.
And now comes the classic question:
“Which one is better, stronger, more powerful, more painful… which one will make me more of a Superman or Spider-Man?”
All those funny (and slightly ridiculous) questions that honestly never cease to amaze me. But here’s the truth: Testosterone is always just testosterone. Those names — propionate, cypionate, enanthate, undecanoate — only describe the ester, which determines how fast the testosterone is released into the bloodstream and how long it remains active in the body after injection.
It’s basically the same as vitamin C — you can have the regular one (no ester) or the slow-release form (with an ester). In the end, it’s still the same vitamin C in your blood, providing the same effects. Of course, there are minor differences between the esters, but for a beginner, that’s not important at all. So forget those questions about which one is stronger — they’re equally effective. Just choose the one you prefer, and over time you can try both esters to see which one suits you better.
5. Sustanon
A mixture of four testosterone esters — not a bad option, but not ideal either. Many beginners choose it because they think that “the more esters, the better” — and while that sounds great on paper, the reality is different. Each ester releases at a different speed, which causes significant fluctuations in blood testosterone levels over time. If you want to minimise that, you need to inject Sustanon every 3–4 days, not once every 5, 6, or 7 days — as most people tend to do.
6. Testosterone Undecanoate (Nebido)
Generally not suitable for hypertrophy, because it doesn’t create the right conditions for an anabolic environment:
Very slow release
Very slow onset of action
Provides stable but low testosterone levels in the blood
This ester is intended exclusively for medical use and TRT (Testosterone Replacement Therapy), as it was designed to mimic the natural testosterone production in a healthy male.

Testosterone Enanthate or Testosterone Cypionate
Injectable cycle for beginners
As I already mentioned, this is the most suitable alternative. Ideally, the injection should be applied once every 4 to 5 days, so that the weekly dose is in the range of 200 to 300 mg. A stable testosterone level in the blood is reached after approximately 4 to 5 half-lives, which for TST E and TST C is roughly after 3–4 weeks — until then, you won’t feel much. The full onset of effects will be noticeable around week 4 to 6,which is why a cycle with TST E or TST C usually lasts 8 to 12 weeks.
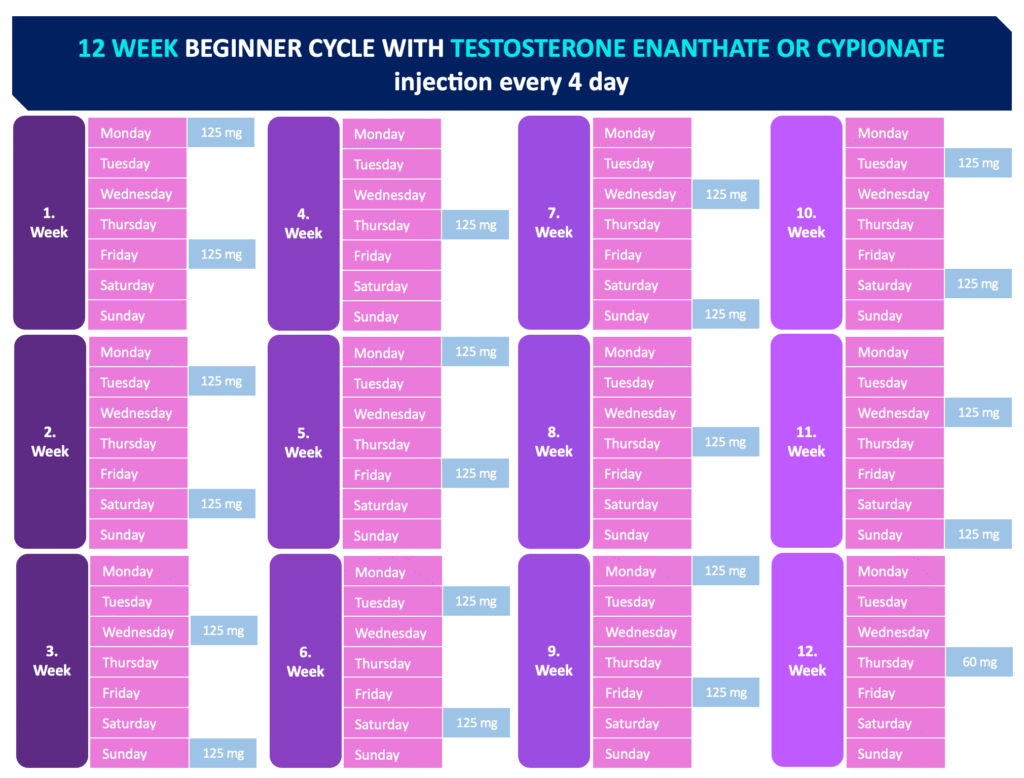
In the table, a dose of 125 mg every 4 days is used, which represents an average weekly dose of 230 mg. The dose can be adjusted to 150 mg, which would represent an average weekly dose of 275 mg.
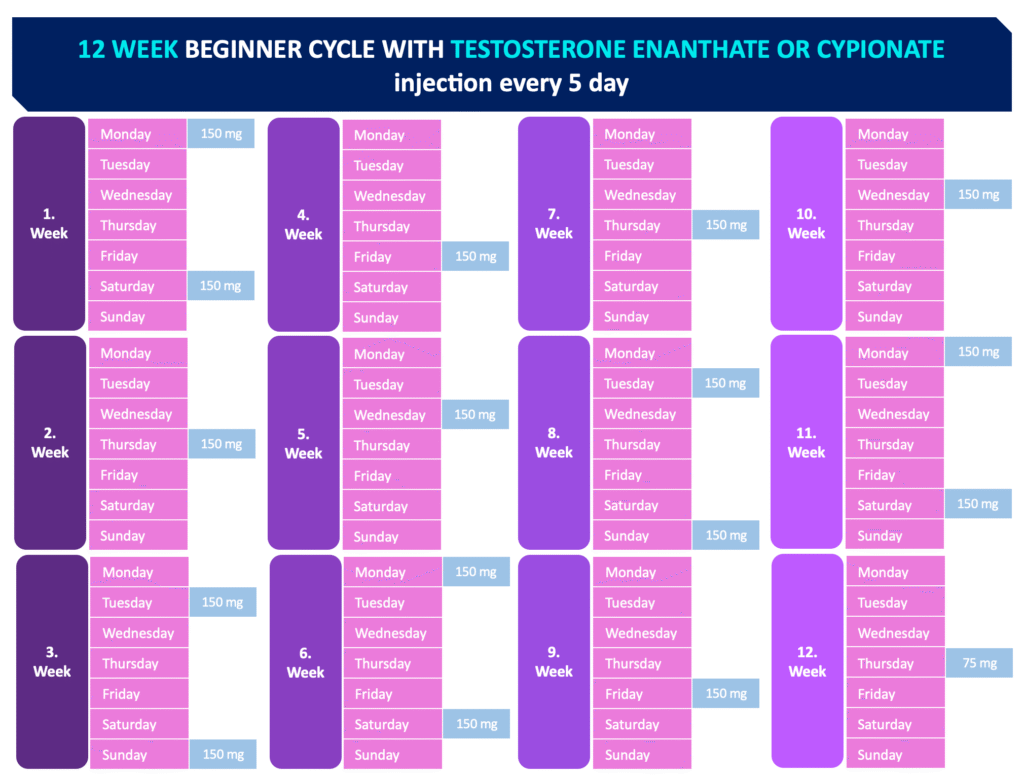
In the table, a dose of 150 mg every 5 days is used, which represents an average weekly dose of 230 mg. The dose can be adjusted to 185 mg, which would represent an average weekly dose of 280 mg.
TST Propionate
Injectable cycle for beginners
The second most suitable option is TST P, which must be injected every day or every other day, so that the weekly dose stays within 200 to 300 mg. A stable blood level is reached after 7–10 days from the first injection — until then, you won’t feel much, and the full effect starts approximately from the second week. That’s why TST P can be used for a shorter period compared to TST E or C, specifically 6 to 8 weeks, or of course even 10 to 12 weeks if the frequent injections don’t bother you.
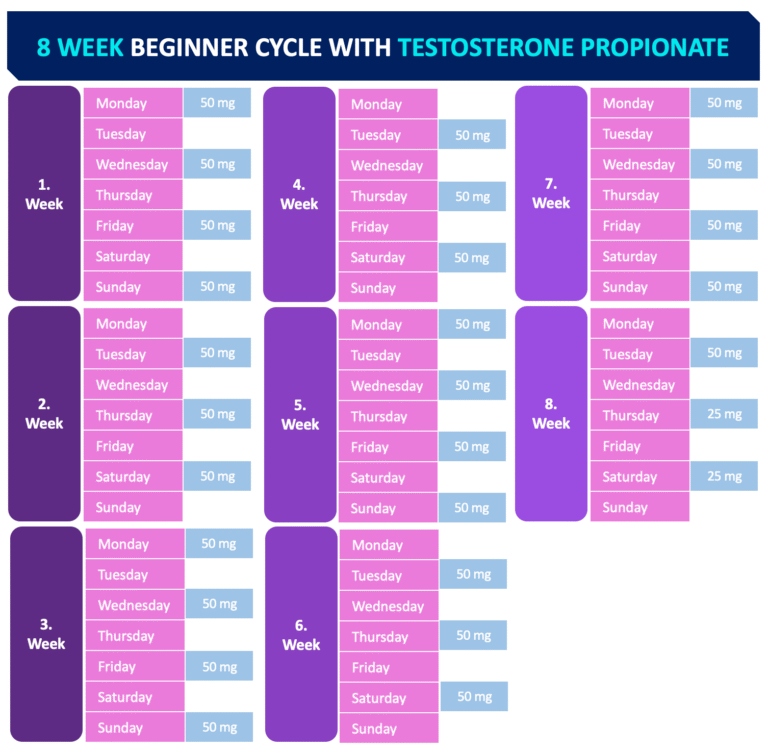
In the table, a dose of 50 mg every other day is used, which represents an average weekly dose of 175 mg. The dose can be adjusted to 75 mg, which would represent an average weekly dose of 260 mg.
Sustanon
Injectable cycle for beginners
The least suitable option is Sustanon, because it contains four different esters,which causes testosterone levels in the blood to fluctuate.To achieve more stable levels, it should also be injected once every 3 to 4 days.Because of the mix of esters, it reaches a stable blood level only after 5–6 weeks of use, and the full effect comes around week 7–8, which is why it should be used for 10 to 12 weeks. To make it clear — if you decide to inject it every 5th, 6th, or 7th day,then the stable levels and full effects will come later, and you’ll basically rob yourself of potential muscle gains.
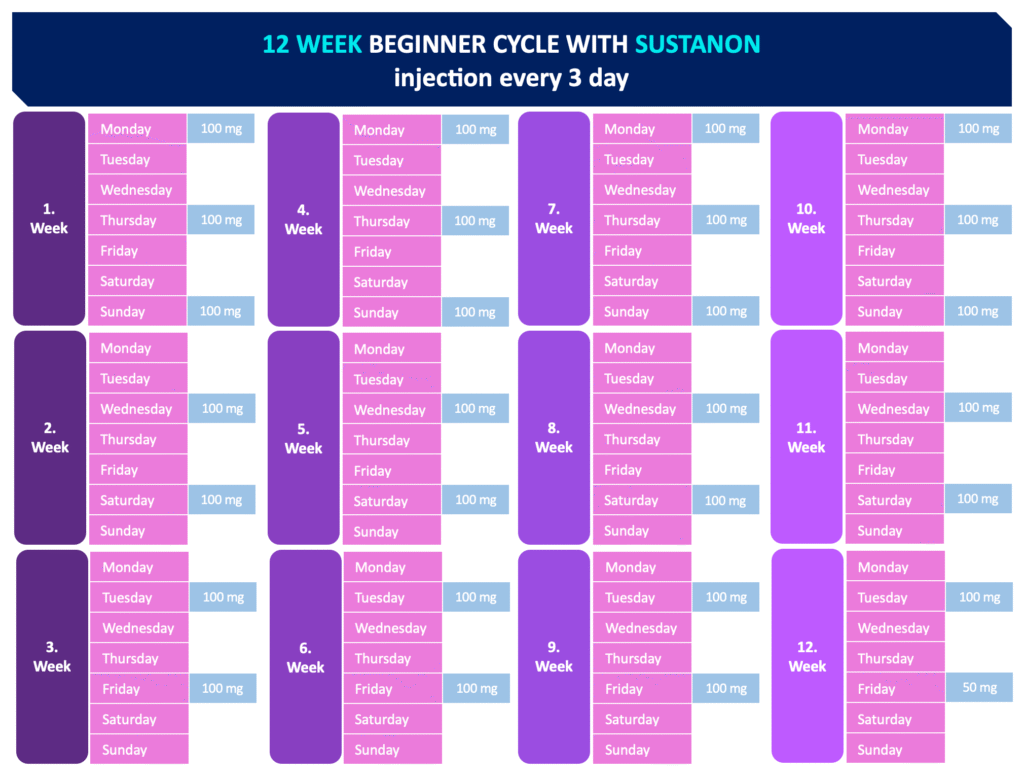
In the table, a dose of 100 mg every third day is used, which represents an average weekly dose of 230 mg. The dose can be adjusted to 125 mg, which would represent an average weekly dose of 290 mg.
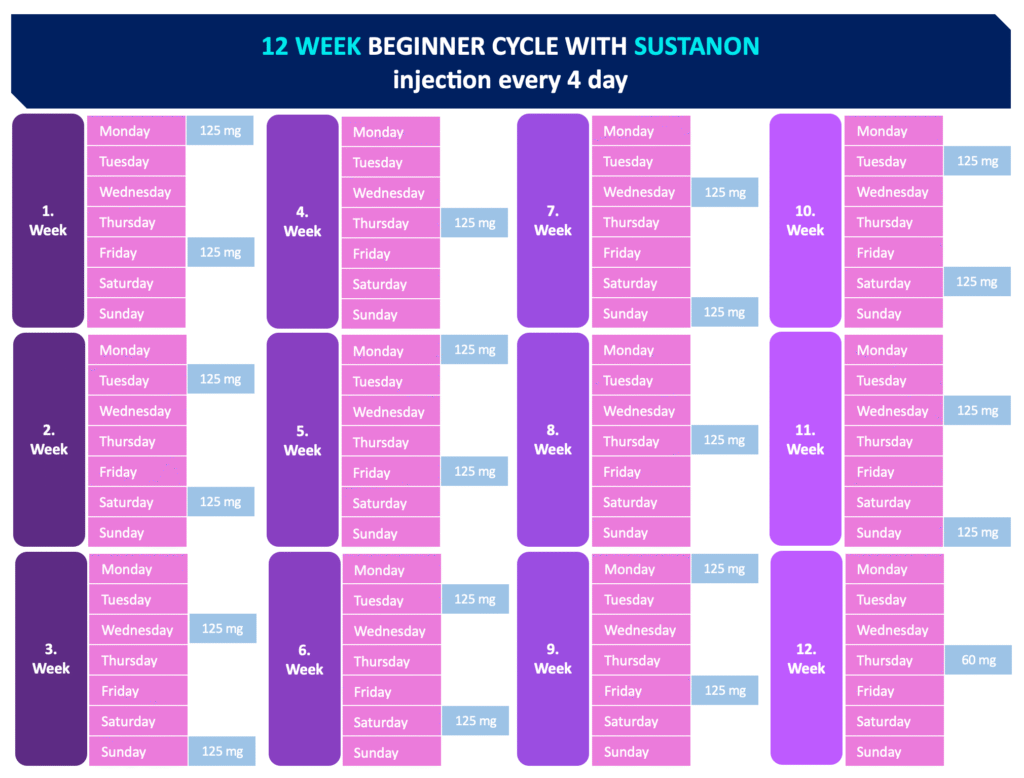
In the table, a dose of 125 mg every fourth day is used, which represents an average weekly dose of 230 mg. The dose can be adjusted to 150 mg, which would represent an average weekly dose of 275 mg.
What is the main advantage of an injectable cycle compared to an oral one?
Minimal liver strain
Higher bioavailability
Fewer gastrointestinal issues
Less negative impact on cholesterol
Injectable cycles can last longer than oral ones
The only real disadvantage I would mention is the injection itself, which is often a psychological barrier for beginners.Of course, injectable AAS also have a slower onset of action.
Estrogen Control
Even in these beginner cycles, it’s essential to monitor your E2 (oestrogen) levels. Almost everyone underestimates this and follows the common but false idea: “I don’t feel anything, so everything must be fine.” Elevated E2 isn’t just about gynecomastia — it can cause many other negative effects, the most concerning being its link to cancer development!Yes, that’s right — chronically elevated E2 levels significantly increase the risk of cancer, both in women and men (for example, prostate cancer). Prolonged high E2 also leads to increased prolactin, which causes sexual dysfunction in men, and more. Simply put, E2 levels must always be kept under control — they can be slightly higher during a cycle but not excessively high. To control it, use Anastrozole or Exemestane. For a weekly testosterone dose of 200–300 mg, most users will do fine with 0.5 mg of Anastrozole every third day or 10 mg of Exemestane every other daythroughout the entire cycle. Of course, it’s assumed that you’re smart enough to understand the need to use HCG during the cycle (250–500 IU every third day), which also raises E2 — therefore, using an aromatase inhibitor (Anastrozole or Exemestane) should simply be a must.
What about after the cycle?
After finishing a cycle, most of you will start PCT (Post Cycle Therapy). Injectable AAS are much more suppressive than oral steroids — they usually shut down natural testosterone production completely (in most cases). That’s why it’s important to use HCG preventively during the cycle, to maintain intratesticular testosterone production and make recovery easier once the cycle ends. After finishing the AAS cycle, you must calculate — based on the half-life of each compound — when to start PCT(Clomid or Tamoxifen). These compounds are only effective when no AAS are left in your bloodstream! With oral AAS, it’s simple — you can start PCT the very next day after stopping. But with injectables, it’s different — you may only start after several days or even weeks, depending on the ester used. There will be a separate article about this topic.
Can I include another injectable AAS in my first cycle besides testosterone?
Many of you ask about a first cycle including Nandrolone, Boldenone, or even just Primobolan. The answer is NO! If you’re starting an injectable cycle, it should always consist of testosterone only. Based on this first, single-compound cycle, you will find out how your body reacts to elevated levels of E2 and DHT, and what positive and negative effects you experience. Only after this basic, first cycle should you consider what to add next. As for Primobolan — yes, it’s often presented as a mild steroid, which is why many of you want to include it in your first cycle. But the same rule applies here as with oral AAS — you need a certain level of oestrogen (E2) to be maintained. Primobolan is a DHT derivative, meaning it has no oestrogenic activity, and your E2 levels will drop sharply during its use, which is simply UNACCEPTABLE! We already explained this in detail in the first part.