

(Nandrolone Decanoate and Phenylpropionate)
To begin, we will briefly familiarise ourselves with Nandrolone as such. It has a very similar chemical structure to testosterone, but from the perspective of hypertrophy it is slightly stronger in comparison — it has a stronger anabolic effect, but milder androgenic activity. It converts into DHN (dihydronandrolone), which, unlike DHT, has a weak affinity for androgen receptors, and that is the reason for its lower androgenic activity compared to testosterone. Nandrolone shows mild oestrogen (E2) activity, compared to testosterone only at around 20%.
Here it is important to understand that Nandrolone does not convert to E2, and overall shows almost zero activity at E2 receptors, but it is able to bind through interaction with specific DNA elements in androgen receptors which carry response elements not only for androgen but also for oestrogen — and this creates the approximately 20% oestrogenic activity of Nandrolone. Which, essentially, is not even important for you. What is important is that Nandrolone accelerates testosterone aromatisation, therefore by itself it has only minimal oestrogen activity, but unfortunately it significantly amplifies the oestrogen activity of testosterone! That is why during any cycle with Nandrolone and testosterone, it is necessary to use an aromatase inhibitor to control E2 levels!
What is the relationship between Nandrolone and prolactin? Nandrolone tends to lower prolactin levels if E2 levels in the blood are low, but if E2 levels rise due to testosterone aromatisation, then there is a high probability that prolactin levels will start to rise quite rapidly! Therefore, as I have already mentioned a million times, during a cycle it is necessary to always keep E2 levels under control through the use of aromatase inhibitors.
Nandrolone has a direct effect on dopamine metabolism, increasing its breakdown ⇒ reducing its levels, which negatively affects cognition, learning, memory. In many users, depressive behaviour, irritability, or reduced motivation can appear. These negative symptoms usually manifest at higher doses or in individuals who naturally have lower dopamine levels, or have an increased predisposition to depression.
Of course, Nandrolone is suppressive to the body’s own testosterone production, but it is not true that it creates long-term or exceptionally strong suppression — this is only a myth, based on the information that Nandrolone can be detectable in the body even 1 year after the last injection. It is true that Nandrolone metabolites can be found in the body long after discontinuation, but they no longer have suppressive effects! After discontinuing Nandrolone, suppression of endogenous testosterone, depending on the dose and ester used (decanoate/phenylpropionate), lasts a maximum of several weeks, certainly not half a year or a year — those are myths.
Nandrolone does not have healing effects on joint injuries, this is another myth! It can create a perceived relief, because it increases fluid retention in the synovial joint. The only thing we can talk about is that Nandrolone increases type I collagen deposition in tendons, which may be beneficial to a certain extent for tendons, but on the other hand this is a negative phenomenon for heart tissue. Nandrolone causes increased deposition of type I collagen in cardiac tissue, leading to its remodelling ⇒ enlargement of the left ventricle and fibrosis (loss of elasticity and thickening, causing functional impairments). Overall, Nandrolone, among all AAS, has exceptionally negative effects on the heart. It also has a significant negative impact on cholesterol levels, its cardiotoxicity is substantial.
“Deca-dick” is a commonly feared effect during Nandrolone use. What is it? It refers to erection problems. Why does it happen? I won’t go into deep detail, as that would take too long, because a combination of factors plays a role here (such as reduced NO availability, cellular damage through oxidative stress, conversion of Nandrolone to DHN instead of DHT, etc.). What matters for you is to keep oestrogen levels from testosterone conversion under control, and by doing so you will automatically keep prolactin under control, which will, in 90% of cases, eliminate sexual issues during Nandrolone use.

Nandrolone is most commonly available on the market with two esters:
1. Nandrolone Decanoate (ND)
-
Half-life: 7 to 10 days
-
It is usually administered once every 3 to 7 days, most commonly in practice once every 4 to 5 days.
-
ND produces muscle gains slowly, which is why cycles with it are long-term, typically 10 weeks or more. A stable blood level of Nandrolone, when administered once every 4 or 5 days at a constant dose, can be reached after approximately 6 to 7 weeks, and its full effect is achieved somewhere around the 8th to 10th week of regular use. However, after roughly 4 to 6 weeks of use, improved recovery, gradually increasing strength, and hypertrophy with a tendency for continued progress may already be noticed.
-
Its doses in men usually range from 200 to 600 mg per week, although there are users who increase doses to 700–1000 mg per week.
-
In women, it is usually taken at 50 to 100 mg per week, but for how long? If virilisation effects start appearing around the 4th to 6th week, it is necessary to decide what to do next — either the dose is reduced or ND is discontinued.
2. Nandrolone Phenylpropionate (NPP)
-
Half-life: 2 to 3 days
-
It is usually administered every second to every third day.
-
NPP produces muscle gains faster than ND, because it has a much shorter half-life, and therefore it can be used even in shorter cycles of 8 or more weeks. A stable blood level with NPP, when administered every second or third day, is achieved after approximately 2 to 3 weeks of use. Maximum effect begins to appear after roughly 4 to 6 weeks of use.
-
Its doses in men are the same as with ND, 200 to 600 mg per week (in exceptional cases 700 to 1000 mg per week).
-
In women, it is usually taken at 50 to 100 mg per week.
What is the correct ratio of Testosterone to Nandrolone?
This has been the subject of discussion for years on various forums. So let’s explain it — we have 3 options:
-
Lower dose of Testosterone and a higher dose of Nandrolone
-
Equal doses of both compounds
-
Higher dose of Testosterone and a lower dose of Nandrolone
Which ratio is correct? All of them are correct, but each has its own specific advantages, and we will describe them in a moment.
1. Lower Testosterone Dose and Higher Nandrolone Dose
This combination is suitable for individuals who have issues with aromatisation in general. Nandrolone itself does not convert to estrogen (E2) and has only very mild estrogenic activity (as explained at the beginning of the article). However, it significantly accelerates the aromatisation of testosterone into E2. Naturally, increased E2 levels bring the risk of gynecomastia and will also raise prolactin levels, which can negatively impact sexual function.
How does such a cycle typically look in practice?
-
100–150 mg Testosterone + 300 mg Nandrolone
-
200 mg Testosterone + 400 mg Nandrolone
-
250 mg Testosterone + 500–600 mg Nandrolone
Even those of you who think you need high doses of testosterone to maintain sufficient libido during a cycle are mistaken — such low doses are completely sufficient. This approach is also suitable for individuals who do not respond well to testosterone and therefore benefit from using it at lower doses. It is also appropriate for those who are prone to hair loss, since nandrolone has only a mild effect on hair. This method of use is also applied in HRT (hormone replacement therapy).
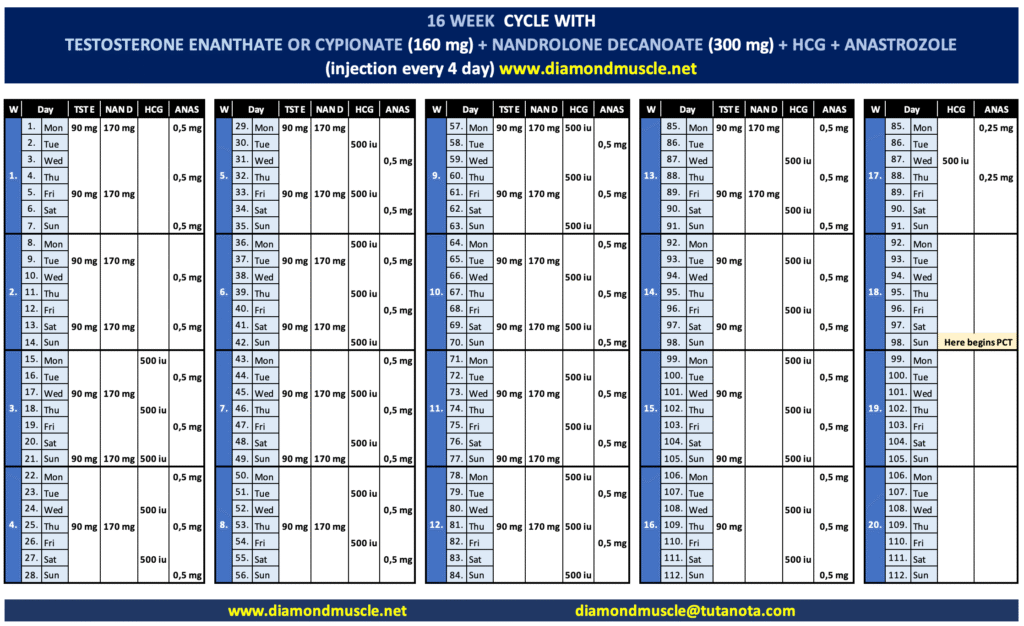
Here you can see an example of a 16-week cycle with Testosterone Enanthate (160 mg per week) and Nandrolone Decanoate (300 mg per week), requiring injections every fourth day, where you draw 90 mg of Testosterone Enanthate + 170 mg of Nandrolone Decanoate together into one syringe each time. During the cycle, HCG is of course used (to support intratesticular production of testosterone, pregnenolone, DHEA, etc.), as well as the aromatase inhibitor Anastrozole (to control E2). As you can see, Nandrolone Decanoate is discontinued significantly earlier than Testosterone Enanthate, because it remains active in the body for quite a long time (approximately 5 weeks after the last dose) and this is necessary for correct PCT timing. If you were to add one more dose, the entire PCT would need to be delayed, since there would still be a high amount of Nandrolone Decanoate in the bloodstream, which would continue to exert suppressive effects. Therefore, PCT begins on Day 98, when the levels of Nandrolone Decanoate (after ~5 weeks) and Testosterone Enanthate (after ~15–16 days) are sufficiently low not to exert suppression.
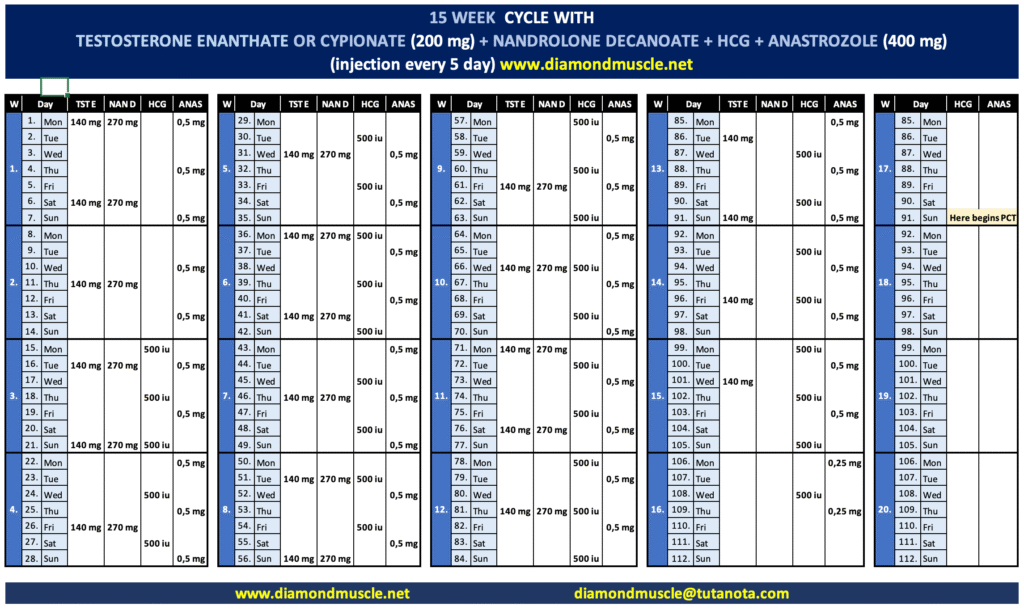
Above, I described the cycle in detail — from now on, each following cycle will be summarized more briefly. The cycle lasts 15 weeks, with an average weekly dose of 200 mg of Testosterone Enanthate and 400 mg of Nandrolone Decanoate. Injections are administered every fifth day (each time drawing 140 mg of Testosterone Enanthate and 270 mg of Nandrolone Decanoate into one syringe). The cycle includes HCG and Anastrozole for the same reasons as in the previous cycle. Also, Nandrolone Decanoate is discontinued earlier than Testosterone Enanthate to create the right environment for proper PCT, which begins on Day 91.
2. Equal dose of Testosterone and Nandrolone
One of the most common ways of using these two compounds is when the user chooses the same dose in mg for both. This ratio can be chosen by anyone who has had a good experience with testosterone use and does not experience significant oestrogen-related side effects, and at the same time does not have issues with reduced dopamine levels when using nandrolone.
In practice, it may look like this:
• 250 mg Test + 250 mg Nandrolone
• 300 mg Test + 300 mg Nandrolone
• 400 mg Test + 400 mg Nandrolone
• And so on
I also recommend monitoring E2 (oestrogen) levels even with a 1:1 ratio, because if they remain elevated for a longer period, it is very likely that prolactin will also increase — an undesirable effect that may lead to gynecomastia issues or sexual-function problems.
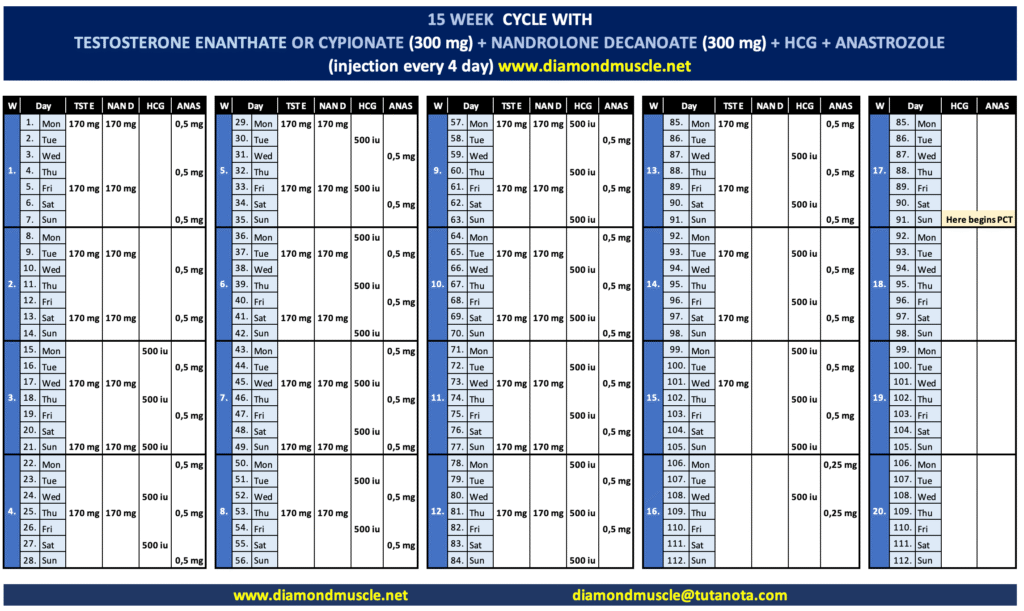
This cycle lasts 15 weeks, with an average weekly dose of 300 mg of Testosterone Enanthate and 300 mg of Nandrolone Decanoate. Injections are administered every fourth day, drawing 170 mg of Testosterone Enanthate and 170 mg of Nandrolone Decanoate into one syringe each time. The cycle includes HCG and Anastrozole for the same reasons as in the previous cycles. Nandrolone Decanoate is also discontinued earlier than Testosterone Enanthate to create an optimal environment for proper PCT, which begins on Day 91.
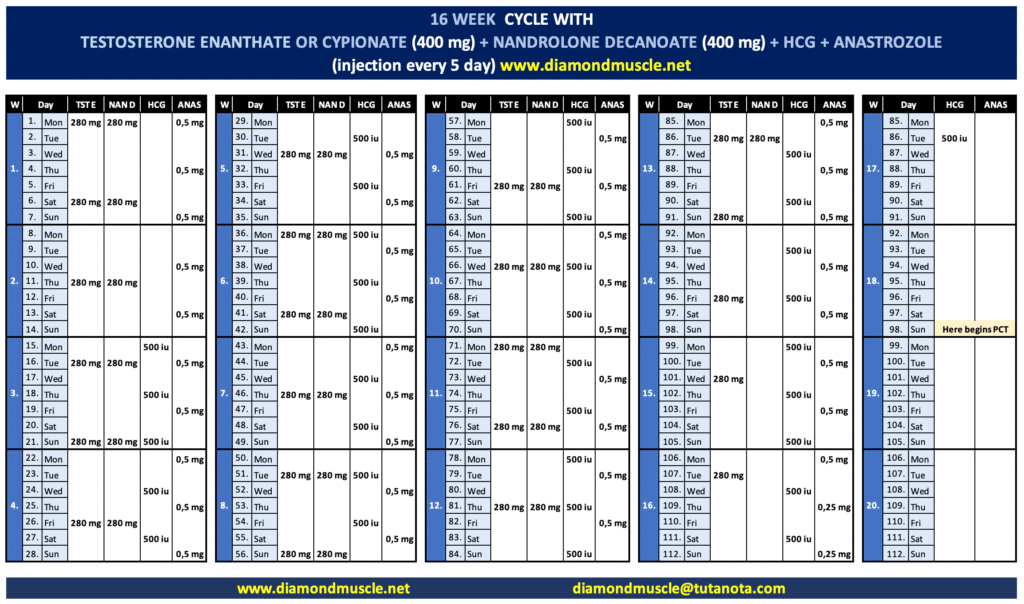
This cycle lasts 16 weeks, with an average weekly dose of 400 mg of Testosterone Enanthate and 400 mg of Nandrolone Decanoate. Injections are administered every fifth day, drawing 280 mg of Testosterone Enanthate and 280 mg of Nandrolone Decanoate into one syringe each time. The cycle includes HCG and Anastrozole for the same reasons as in the previous cycles. Nandrolone Decanoate is also discontinued earlier than Testosterone Enanthate to create an optimal environment for proper PCT, which begins on Day 98.
Higher dose of Testosterone and lower dose of Nandrolone
This ratio is suitable for those who respond poorly to nandrolone as a compound that directly increases dopamine breakdown (lowers dopamine). This negatively affects cognition, focus, learning, memory, mood and sexual function. In some individuals, this effect can become quite pronounced.
It is also suitable for those who want perceived relief from joint pain — note, nandrolone does not heal joint injuries! It only provides subjective relief. Additionally, this ratio is appropriate for individuals who struggle with elevated haematocrit. Nandrolone is a strong erythropoietic compound, so lower doses are more favourable in this regard.
In practice, it may look like this:
• 200 mg Test + 100 mg Nandrolone
• 300 mg Test + 150 mg Nandrolone
• 400 mg Test + 200 mg Nandrolone
• 500 mg Test + 250 mg Nandrolone
As with all combinations, it is essential to monitor E2 levels, because neglecting them during nandrolone use may lead to an increase in prolactin, which is an undesirable effect.
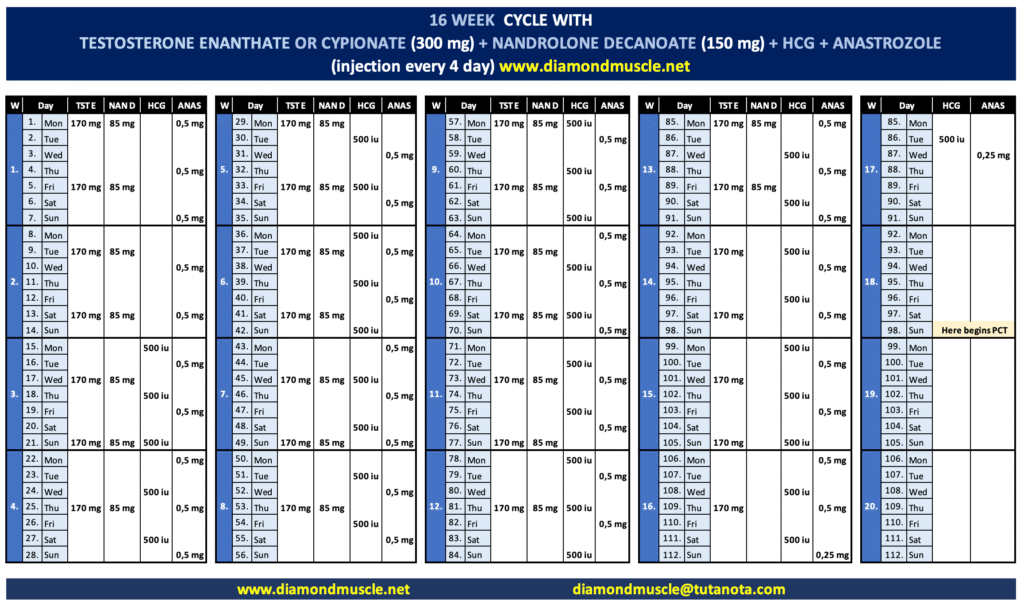
This cycle lasts 16 weeks, with an average weekly dose of 300 mg of Testosterone Enanthate and 150 mg of Nandrolone Decanoate. Injections are administered every fourth day, drawing 170 mg of Testosterone Enanthate and 85 mg of Nandrolone Decanoate into one syringe each time. The cycle includes HCG and Anastrozole for the same reasons as in the previous cycles. Nandrolone Decanoate is also discontinued earlier than Testosterone Enanthate to create an optimal environment for proper PCT, which begins on Day 98.
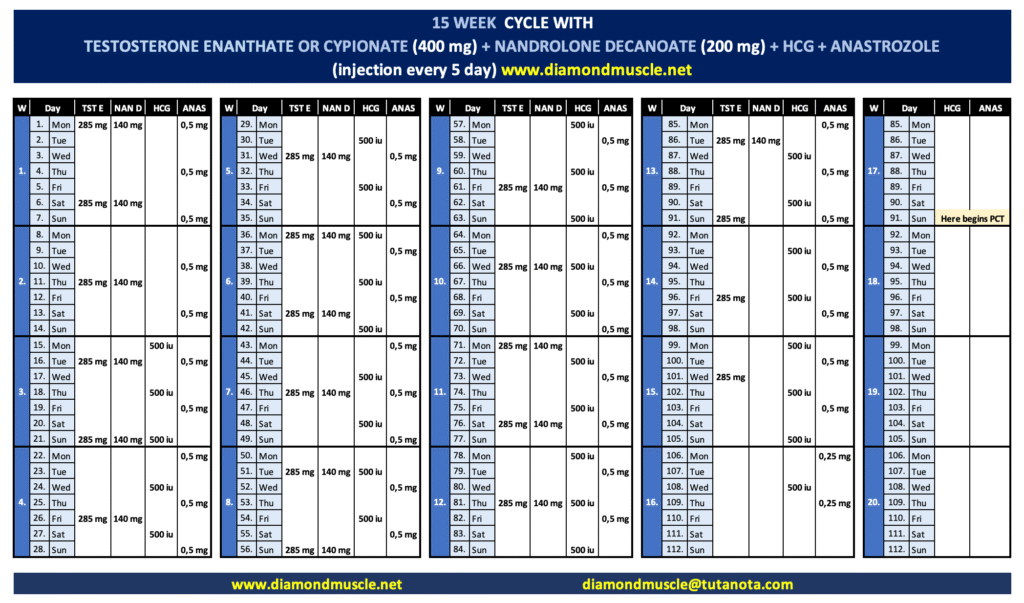
This cycle lasts 15 weeks, with an average weekly dose of 400 mg of Testosterone Enanthate and 200 mg of Nandrolone Decanoate. Injections are administered every fifth day, drawing 285 mg of Testosterone Enanthate and 140 mg of Nandrolone Decanoate into one syringe each time. The cycle includes HCG and Anastrozole for the same reasons as in the previous cycles. Nandrolone Decanoate is also discontinued earlier than Testosterone Enanthate to create an optimal environment for proper PCT, which begins on Day 91.
As you have seen, all combinations are correct and each has its purpose, so next time you don’t need to argue with your friend about which one is better. Simply choose the one that suits your needs.
I would like to emphasise one thing: If you decide to monitor E2 levels through blood tests while using Nandrolone, they will always appear “high”, because Nandrolone causes falsely elevated E2 values in standard blood tests. Only if you have access to the more sensitive ECLIA test will you get accurate E2 results. Therefore, measuring E2 levels during Nandrolone use with regular blood tests makes no sense.