Have you decided to start using AAS and are now wondering what to include in your first cycle?
You have three basic options:
-
Oral cycle
-
Injectable cycle
-
Combination (injectable + oral)
But before we go any further, let’s answer some essential questions most beginners tend to ask themselves:
1. WHEN TO START?
Ideally — never! But if you’ve already made up your mind, then the later, the better. There’s no exact age when you can say, “now is the right time.” Generally speaking, starting before the age of 20 is far too early, and if you really decide to do it, it should be somewhere between 25 and 30 years old.
It’s important to note that if you don’t know how to train properly, don’t understand what it means to train to failure, don’t have a solid diet, or don’t know what it means to eat until you feel sick, then even thinking about using AAS is a really bad idea. Without honest, consistent training and quality nutrition, AAS simply can’t do their job!
2. HOW LONG SHOULD THE CYCLE LAST?
The shorter, the better — especially if your cycle includes too many oral compounds. In general, beginner cycles usually last between 6 and 12 weeks.
3. WHAT TO DO AFTER THE CYCLE?
After completing a cycle, the focus should be on restoring your natural testosterone production and sperm count. The goal is also to preserve as much muscle mass as possible — although this is almost impossible, and most people will lose the majority of their newly gained muscle within a short time. Yes, unfortunately, that’s the harsh reality! And that’s exactly why many users soon fall into another cycle… and then another, and another.

ORAL CYCLE
Beginners often choose an oral-only cycle mainly because they are afraid of needles and the idea of injecting themselves. However, today we know that injectable AAS can be administered using an insulin syringe with a thin needle only 0.5–1 cm long, injected subcutaneously (under the skin or into fat). It’s a virtually painless application, barely noticeable, and there’s absolutely no need to use a “thick” 3 cm needle. Still, if you are genuinely afraid of injections, there is always the option of a purely oral cycle.
DISADVANTAGES OF AN ORAL CYCLE
-
High hepatotoxicity (increased liver stress)
-
Negative impact on cholesterol (reduction of HDL, increase in LDL and triglycerides)
-
Limited duration of use (4 to 10 weeks)
-
Irritation of the stomach lining and increased acid production (heartburn, reduced appetite)
ADVANTAGES OF AN ORAL CYCLE
-
Fast onset of effects and easy administration
-
Less suppression of natural testosterone production compared to injectable AAS (recovery of natural testosterone levels after stopping oral AAS is easier and faster)

WHAT TO INCLUDE IN YOUR FIRST ORAL CYCLE?
What I’m about to explain is something that even many long-term AAS users don’t fully understand.
A lot of beginners make a fundamental mistake by including compounds such as Stanozolol, Oxandrolone, Turinabol, or Methyldrostanolone in their first cycle.
These are not the right choice! Why? Because they are DHT derivatives with no oestrogenic activity. The male body needs oestrogen (E2), which is naturally produced from testosterone.
If you start using the substances mentioned above, your own testosterone production will drop by at least 50% or more, which means your E2 levels will also fall below normal reference ranges.
What are the consequences of low E2 levels?
-
Irritability, depression, emotional numbness (low E2 has a strong negative impact on serotonin and dopamine)
-
Cardiovascular issues and worsened lipid profile (E2 protects the heart and blood vessels, increases HDL and reduces LDL)
-
Poor recovery, fatigue, and joint, tendon, and muscle pain
-
Reduced bone mineralisation
-
Lower sexual libido, decreased penile sensitivity, reduced androgen receptor sensitivity, and lower levels of IGF-1 and growth hormone
Methandienone – the Most Common and Best Choice for Beginners
Why? Because it is a testosterone derivative that possesses oestrogenic activity — which is essential for maintaining hormonal balance.
A dose as low as 10 mg per day is enough to fully replace the body’s natural daily testosterone production. What does this mean? You won’t experience issues with libido, and your sexual function will remain completely normal. Its negative effect on cholesterol is also less pronounced compared to the AAS compounds mentioned earlier, precisely because of its oestrogenic activity. However, its hepatotoxicity (liver stress) is similar to that of other oral AAS.

Typical Dosage for Beginners
The daily dose usually ranges from 20 to 30 mg for a duration of 6 to 8 weeks (sometimes up to 10 weeks). The daily amount should be split into 2 or 3 doses, as Methandienone (Dianabol) has a very short half-life of about 2.5 to 5 hours.
In practice, this can look like:
-
10 mg in the morning
-
10 mg in the evening
or
-
10 mg in the morning
-
10 mg in the afternoon
-
10 mg in the evening
You can either choose a constant daily dose from the start — for example, 20 mg per day throughout the entire cycle — or you can use a titration approach. What does titration mean? Titration means adjusting your daily dose according to your needs, side effects, and overall satisfaction with results.
For instance:
-
Week 1: 20 mg/day
-
Week 2: 25 mg/day
-
Week 3: 30 mg/day
And you can continue at that dose until the end of the cycle, or reduce it again to 25 mg or 20 mg whenever needed. It’s always a good idea to gradually taper down the dose at the end of the cycle rather than stopping abruptly. For example, during the last 3–4 days, reduce the dosage pyramid-style: 30 → 25 → 20 → 10 mg.

What to Do After the Cycle (PCT)? What to Focus On?
Ideally, you should start Clomid at a low dose of 25–50 mg per day for a period of 4 to 6 weeks, beginning the day after stopping Methandienone (MET). Methandienone can significantly suppress natural testosterone production, but it doesn’t completely shut it down like injectable AAS do — which means recovery is generally easier and faster.
As an alternative, you can use Tamoxifen at a daily dose of 10–20 mg, but from my perspective, Clomid is the better choice. If you decide to go with either Clomid or Tamoxifen, they should be taken in the morning as a full single dose.
At the same time, it’s beneficial to include GHRP-2, GHRP-6, or other GHRP/GHRH peptides to support anabolic processes and recovery after discontinuing MET.
GHRP-6/ GHRP-2 should always be taken on an empty stomach, ideally three times per day at a dose of 100 mcg each time (morning, afternoon, and evening) — for a total of 300 mcg per day. It is administered subcutaneously (under the skin or into fat) using an insulin syringe, which makes the application comfortable and easy. If injecting three times a day feels too demanding, it can also be taken twice daily at 100 mcg per injection, for a total of 200 mcg per day, applied in the morning and in the evening.
You’ll probably ask what the difference between GHRP-2 and GHRP-6 is — and which one to choose. The only real difference is that GHRP-6 tends to increase appetite more noticeably during the first 7 to 14 days, while GHRP-2 has a much milder effect in this regard. Otherwise, you can choose any other GHRH or GHRP peptide, or even a combination of both. I’ve simply outlined the core idea here — it’s up to you to work with it further based on your own goals and experience.
After completing PCT, you can either choose to never use AAS again — or start another cycle later on.

A Note on Oestrogenic Effects and Gynecomastia Prevention
Before I forget — some of you may experience stronger oestrogenic effects, while others may not notice them at all. That’s why it’s important to have a SERM (anti-oestrogen) such as Tamoxifen or Raloxifene readily available. I strongly recommend having it on hand from the start of the cycle, not buying it later when it might already be too late.
Think of it as a useful long-term investment — even if you don’t need it during this cycle, you may find it necessary in a future one. To be clear, we’re talking about the potential development of gynecomastia. It’s highly unlikely to occur at daily doses of 20–30 mg for most of you. Those most prone to developing gynecomastia are younger men under 25, and on the other side, older users, since oestrogen sensitivity increases with age, especially after 50.
If a Problem Occurs
If you notice small lumps or nodules under your nipples that are painful or sensitive to the touch, it’s time to start Tamoxifen or Raloxifene alongside your current cycle.
-
If you choose Tamoxifen, begin with 20 mg per day until the issue subsides (typically about 10 days). Then reduce the dose to 10 mg, and later to 5 mg, depending on your symptoms and oestrogenic response.
-
If you opt for Raloxifene, the same principle applies — start with 60 mg per day for about 10 days. Once the sensitivity disappears and the lumps begin to shrink, lower the dose to 30 mg per day, and continue until the end of the cycle.
Many of you tend to worry excessively about gynecomastia, but keep in mind — it doesn’t develop overnight. It’s a slow, gradual process. During AAS use, you may notice mild nipple sensitivity or slight gland enlargement — this is a normal and temporary reaction, not true gynecomastia. Often, frequent touching and checking the area amplifies the sensitivity, leading you to believe something’s wrong when it isn’t.
So, unless the sensitivity continues to worsen and actual lumps form, there’s no need to start SERMs immediately. If you choose a 6- or 8-week Methandienone cycle with doses up to 30 mg per day, the risk of developing gynecomastia is minimal for the vast majority of users.

Combining Orals – Yes or No?
Of course, it’s possible to combine oral compounds, but the foundation of any cycle should always be Methandienone (MET) — though in this case, at a lower dose of 10 mg per day. This serves to maintain sexual function and ensure adequate oestrogenic activity. The daily dose of Methandienone is divided into 2 × 5 mg — one in the morning and one in the evening.
You can then add one of the following compounds alongside it:
-
Stanozolol
-
Oxandrolone
-
Turinabol
However, as a beginner, you should avoid more potent androgens such as Oxymetholone, Methyldrostanolone, or Fluoxymesterone.
When I first published these types of beginner-friendly cycles, they received quite a bit of criticism from a few less-informed individuals, with comments like “So every cycle includes Methandienone — what’s the point?”
Let me be blunt for a moment — if you don’t understand the basics, you shouldn’t be commenting on it. Yes — every cycle includes MET for a reason: to maintain essential sexual function and preserve necessary oestrogenic activity. As I’ve already mentioned, a daily dose of 10 mg of Methandienone fully replaces the body’s natural daily testosterone production, from a medical standpoint. That’s because Methandienone was originally developed by scientists as an oral substitute for injectable testosterone.
Example Combination Cycles
1. MET + Stanozolol
The daily dose of Stanozolol for beginners typically ranges between 20–30 mg per day. It is divided into two doses — either 2 × 10 mg or 2 × 15 mg. Stanozolol is stronger than both Oxandrolone and Turinabol. It is usually taken for 4 to 8 weeks, and in exceptional cases up to 10 weeks, if using lower doses.
2. MET + Oxandrolone
The daily dose of Oxandrolone for beginners usually ranges from 30 to 40 mg per day, split into 2 doses of 2 × 15 mgor 2 × 20 mg.
Most users prefer 40 mg per day due to Oxandrolone’s weaker anabolic potential. It is a milder compound compared to Stanozolol, but be careful — in terms of cardiovascular side effects, Oxandrolone is actually worse.
It has a stronger negative effect on cholesterol levels and is similarly hepatotoxic (liver toxic) as Stanozolol. I’m mentioning this because myths still circulate suggesting that Oxandrolone is a “mild” steroid.
This statement needs to be properly understood — yes, it’s mild in the sense that it’s a weak androgen and causes moderate muscle gains, but in terms of hepatotoxicity and cardiotoxicity, it is not mild at all! It is commonly used for 4 to 8 weeks, and in rare cases up to 10 weeks at lower doses.
3. MET + Turinabol
Very few beginners choose this combination, mainly because Turinabol is not as popular marketing-wise.
In terms of anabolic potential, it sits above Oxandrolone but below Stanozolol. The daily dose for beginners typically ranges between 20–30 mg, most commonly 30 mg per day, split into 2 doses of 15 mg each. It is typically used for 4 to 8 weeks, and in exceptional cases up to 10 weeks at lower doses.
Its negative effect on the liver is comparable to other oral AAS, and it is also cardiotoxic in terms of cholesterol impact.
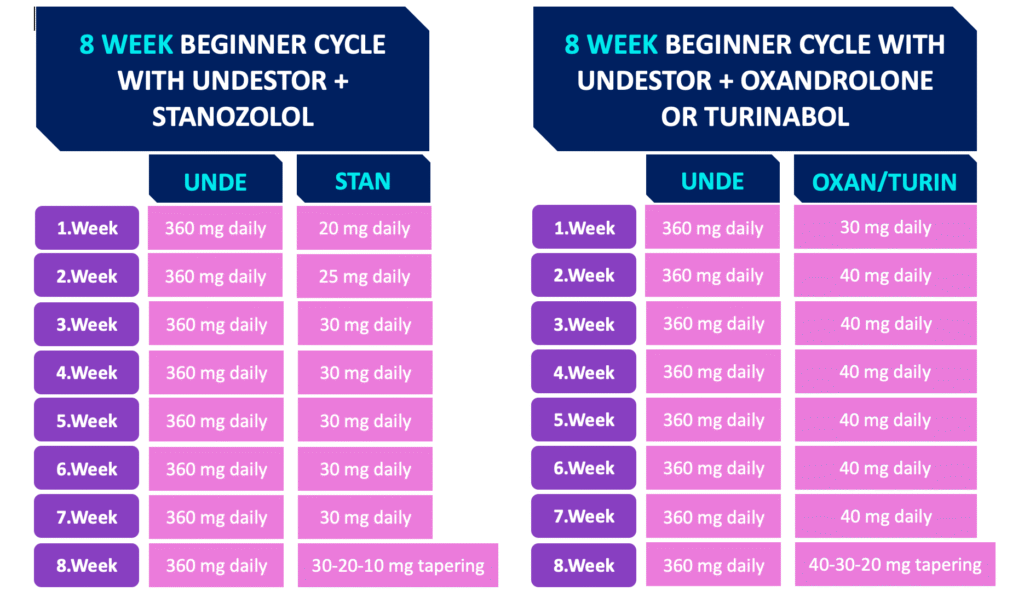
Below you can see an example of how such a cycle could look in practice.
I haven’t created a separate version for Turinabol, as its structure is identical to that of Oxandrolone.

And what about Testosterone Undecanoate (Undestor) in oral form as the base of a cycle instead of Methandienone?
Yes, it’s actually quite a good choice — and if you have access to it, go ahead. It helps maintain sexual function and also provides the necessary oestrogenic activity. It should be taken in a daily dose of 240 mg or more per day, which is really the minimum (meaning 6 or more capsules containing 40 mg of active substance each).
Its main advantage is that it’s minimally toxic to the liver, as it’s absorbed through the lymphatic system — unlike all other AAS. Now you’re probably thinking: “Great, I’ll just use Undestor instead of Methandienone, right?”
Well, let’s go through the disadvantages:
1. Very low bioavailability
It has only minimal biological availability — around 10% — which makes it quite inefficient. That’s exactly why it’s no longer used in modern medicine.
2. Must be taken with food containing fat
It must always be taken together with a meal that contains enough fat, otherwise it won’t be absorbed at all, and its effectiveness drops even further.
3. High dosage requirement
Because of its poor absorption, you’ll need to take very high doses (240 mg or more per day).That means you’ll go through several packs per cycle, which will make your cycle significantly — really significantly — more expensive!
How to properly use Testosterone Undecanoate (Undestor):
-
Always take it with a meal that contains some fat, otherwise it will be ineffective.
-
It has a short half-life (2–5 hours) — after proper administration, blood testosterone levels rise within 4–6 hours, and after about 8–10 hours, they drop back to baseline.Therefore, the daily dose must be split into at least 2–3 portions.
- The minimum daily dose is 240 mg or more, ideally 360 mg, divided as follows:
- 120 mg in the morning with food
- 120 mg in the afternoon with food
- 120 mg in the evening with food
Example cycles with Undestor:
-
Testosterone Undecanoate (Undestor) + Stanozolol
-
Testosterone Undecanoate (Undestor) + Oxandrolone
-
Testosterone Undecanoate (Undestor) + Turinabol